As a local insurance expert helping retirees from Phoenix to Tucson, and across the Valley, I’m seeing a big shift this year. Many of my neighbors are asking if they should stick with a Medicare Advantage plan. While those “zero-premium” ads are everywhere in Arizona, there’s a lot they don’t tell you.
After reviewing the latest industry updates, I’m personally recommending Medicare Supplement Plan G for those who want total freedom and financial peace of mind. Here is why:
1. I want you to have “No-Hurdle” healthcare ? A major issue with many plans right now is “prior authorization”—where the insurance company has to approve a procedure before you can get it. This causes delays that none of us want. With Plan G, if Medicare covers it, your supplement pays. I want the decision-making in your doctor’s hands, not a corporation’s.
2. See any doctor in Arizona (and the U.S.) ? I hate seeing my clients limited by restricted networks. Whether you want to see a specialist at the Mayo Clinic in Scottsdale, a provider in Flagstaff, or even a doctor while visiting family back east, Plan G lets you go anywhere that accepts Medicare.No networks, no “out-of-network” penalties.
3. The ultimate “Snowbird” protection ✈️ Many of my clients in Mesa, Surprise, and Sun City split their time between states. Advantage plans are often tied to your local Arizona zip code.Because Plan G is nationwide, your coverage is just as strong in the Midwest as it is here in the desert.
4. No “Surprise” medical bills ? Advantage plans often have co-pays for every visit and hospital stay. I prefer the predictability of Plan G. Once you meet the small annual Part B deductible ($283 in 2026), your out-of-pocket costs for Medicare-covered services are zero. No more worrying about what the mail will bring after a doctor’s visit.
Your health deserves more than a “pay-as-you-go” plan. If you live in Scottsdale, Chandler, Peoria, or anywhere in the Grand Canyon State, let’s talk about how to protect your retirement.
? Give me a call today to discuss your 2026 options!
If you’re shopping for ACA health insurance in Arizona for 2026, you’ve likely noticed two major changes:
Premiums are significantly higher
Nearly all available plans are HMO-only
For many Arizona individuals, families, and self-employed professionals, this means paying more each month while having fewer choices of doctors and hospitals.
But there are alternatives worth exploring.
Why ACA (Obamacare) Plans Feel So Expensive in 2026 Across Arizona, most 2026 marketplace plans are structured as HMOs. That means:
You must stay in-network
Referrals are often required
Out-of-network care is not covered
Premiums continue to rise year after year
If you don’t qualify for large subsidies — or you’re relatively healthy — you may feel like you’re overpaying for coverage you rarely use.
Many Arizona residents are now looking for PPO alternatives to Obamacare that provide flexibility and affordability.
Catastrophic PPO Plans Are Back in Arizona
Recent regulatory updates have expanded access to catastrophic-style coverage options.
These plans are designed for:
Individuals
Families
Self-employed (1099 earners & small business owners)
Healthy applicants seeking lower premiums
Unlike ACA HMO plans, many of these options operate as PPO networks, giving you broader access to providers without referral restrictions.
PPO Networks Available in Arizona
Several alternative plans use nationally recognized provider networks, including Cigna and Aetna
Blue Cross Blue Shield PPO (Group Plan for Individuals)
One exciting development is access to a group-based PPO plan available to individuals, utilizing the Blue Cross Blue Shield network.
This allows qualifying individuals to access a broad PPO network typically associated with employer group plans — not limited marketplace HMOs.
Why Catastrophic PPO Plans Are So Popular
These plans are structured differently than ACA coverage and can offer major advantages:
Lower Monthly Premiums
Designed primarily to protect against major medical events rather than routine care.
PPO Flexibility
No primary care referral requirements. Greater provider choice.
Fast Start Dates
Coverage can often begin as soon as the next day after approval.
Nationwide Access
Ideal for travelers, snowbirds, and families with children out of state.
Who Should Consider ACA Alternatives in Arizona?
These options may be a strong fit for:
Healthy individuals under 65
Families who rarely hit their deductible
Self-employed professionals
Contractors and 1099 earners
Early retirees not yet eligible for Medicare
If you’re paying high ACA premiums and rarely using your coverage, exploring PPO alternatives may significantly reduce your monthly cost.
Compare Your 2026 Options Before You Renew
Before automatically renewing your ACA marketplace plan, it’s smart to compare:
HMO marketplace coverage
Catastrophic PPO plans
Group PPO options for individuals
Coverage for families and self-employed
You may find better pricing and broader network access than you expected.
Get Personalized Help in Arizona
If you live in Surprise, Phoenix, Peoria, Glendale, Buckeye, Goodyear, or anywhere in Arizona, I’m happy to help you review your options.
Call, email, or text anytime. I’ll provide a side-by-side comparison so you can make the best decision for your health and budget in 2026.
#ArizonaHealthInsurance
#HealthInsuranceArizona
#ArizonaACA
#ACA2026
#ObamacareArizona
#ArizonaPPO
#ArizonaHMO
#ArizonaInsuranceBroker
#SurpriseAZInsurance
#PhoenixHealthInsurance
#PPOInsurance
#CatastrophicHealthPlan
#AffordableHealthInsurance
#ObamacareAlternatives
#HealthInsuranceOptions
#SelfEmployedHealthInsurance
#1099HealthInsurance
#SmallBusinessHealthInsurance
#PrivateHealthInsurance
#SurpriseArizona
#WestValleyAZ
#PhoenixArizona
#PeoriaAZ
#GlendaleAZ
#GoodyearAZ
#BuckeyeAZ
Serving clients throughout Surprise, Phoenix, Peoria, Glendale, Goodyear, Buckeye, and all of Arizona. If you’re searching for an experienced Arizona health insurance broker who can compare PPO and ACA options, contact Andy Orlikoff today.
Many seniors who are 65 and over rely on Medicare to provide them with healthcare coverage, and with good reason. Medicare is available from the government regardless of your health status. It provides coverage for a broad array of services (typically without requiring pre-approval), and it usually comes with affordable premiums.
The keyword, there, however, is usually.
Medicare premiums for most seniors come in at $202.90 for Medicare Part B in 2026. However, some seniors will find themselves hit with an unexpected Medicare surcharge that they may not have been expecting — and that could have a serious impact on their finances. Here’s why these surcharges happen and what it could mean for you.
If your income is $109,000 or higher, you could face a surprise Medicare hit
The Medicare surcharge that you could find yourself surprised by results from something called the Income-Related Monthly Adjustment Amount, or IRMAA.
IRMAA causes your Medicare Part B and Medicare Part D premiums to increase dramatically once your income goes above a specific threshold. That threshold is $109,000 for single tax filers and $218,000 for married joint filers. However, while this is the threshold in 2026 that will send your Medicare premiums surging, it’s not your 2026 income that matters, or even your 2025 income.
The income that matters is your Modified Adjusted Gross Income (MAGI) from two years earlier. So, if your MAGI in 2024 was above those thresholds, then you’ll be faced with higher Medicare premiums in 2026. This can come as a shock, as you may not be aware that a year of higher-than-normal income due to something like capital gains from selling high-performing investments could end up being a ticking time bomb that causes your Medicare premiums to substantially increase two years later.
How much higher will your Medicare premiums go?
The increase in Medicare premiums that results once your income exceeds IRMAA thresholds can be extremely substantial. The table below shows how much you can expect to pay in monthly premiums based on your MAGI and the Income-Related Monthly Adjustment amount:
Full Part B Coverage
Single tax filers with a MAGI that is:
or Joint tax filers with a MAGI that is:
Will pay an IRMAA equal to:
Bringing total Medicare premiums to:
Less than or equal to $109,000
Less than or equal to $218,000
$0.00
$202.90
Greater than $109,000 and less than or equal to $137,000
Greater than $218,000 and less than or equal to $274,000
$81.20
$284.10
Greater than $137,000 and less than or equal to $171,000
Greater than $274,000 and less than or equal to $342,000
$202.90
$405.80
Greater than $171,000 and less than or equal to $205,000
Greater than $342,000 and less than or equal to $410,000
$324.60
$527.50
Greater than $205,000 and less than $500,000
Greater than $410,000 and less than $750,000
$446.30
$649.20
Greater than or equal to $500,000
Greater than or equal to $750,000
$487.00
$689.90
That means you could be looking at paying as much as $487 extra per month — and paying total premiums as high as $689.90 — because you had a year when your income was high. Of course, if you have many years of high earnings as a retiree, you could be hit with this surcharge for the entirety of your retirement during the years Medicare covers you.
What can you do about the IRMAA adjustments?
If you are subject to these adjustments to Medicare premiums because of your income, there’s not much you can do.
Your best bet is try to avoid having this happen in the first place by considering investing for retirement in a Roth IRA or 401(k) instead of a traditional account, and being careful about how large your withdrawals are or when you sell assets to limit capital gains.
A financial advisor can help you make a strategic plan to try to help you avoid sending your Medicare premiums skyrocketing, so you can keep more of your hard-earned funds in your accounts instead of sending extra money to Medicare.
Original Medicare (Parts A and B) is a great start, but it leaves significant “gaps”—like the 20% coinsurance you pay for doctor visits and hospital stays. Medigap Plan G is designed to step in and pay those bills for you, providing the most comprehensive coverage available to new Medicare members today.
How Plan G Works
Think of Plan G as a “shield” for your savings. Once you pay one small annual deductible, your plan takes over 100% of your Medicare-approved medical bills.
You pay the Part B Deductible: In 2026, this is $283 for the entire year.
Plan G pays the rest: After that first $283, you pay $0 for Medicare-approved doctor visits, surgeries, lab work, and hospital stays.
Freedom of Choice: You can see any doctor in the U.S. who accepts Medicare. No networks, no referrals, and no “prior authorizations” required.
Why Plan G is Your Best Option
While other plans exist, Plan G remains the “Gold Standard” for three reasons:
Total Predictability: You’ll never have to guess what a surgery or specialist visit will cost. Your only medical expense for the year (after your premium) is the $283 deductible.
Excess Charge Protection: Some doctors charge up to 15% above the Medicare-approved rate. Plan G is one of the only plans that covers these “Excess Charges” in full.
Travel Peace of Mind: Plan G includes Foreign Travel Emergency coverage, paying 80% of costs for medical emergencies outside the U.S. (up to plan limits).
The Hazard of Waiting: Why Now is the Best Time
There is a “Golden Window” to buy a Medigap plan, and missing it can be a costly mistake.
No Medical Questions Today: When you first turn 65 (or join Part B), you have a 6-month Open Enrollment Period. During this time, insurance companies must sell you a policy at the best price, regardless of your health history.
Medical Underwriting Later: If you wait and try to sign up later, companies can “underwrite” you. This means they can look at your medical records and:
Charge you a much higher monthly premium.
Deny you coverage entirely based on pre-existing conditions like heart disease, diabetes, or even minor health changes.
Locked-In Access: Once you are in a Medigap plan, your coverage is guaranteed renewable. As long as you pay your premium, the insurance company can never cancel your plan because of your health.
CONTINUED ON NEXT PAGE
Plan G vs. The Alternatives
Feature
Medigap Plan G
Medicare Advantage
Doctor Choice
Any doctor in the U.S.
Limited Network (HMO/PPO)
Referrals
Never needed
Usually required for specialists
Out-of-Pocket Costs
$283 annual max
Up to $9,000+ per year
Predictability
High (Flat monthly premium)
Low (Pay-as-you-go copays)
The Bottom Line: If you want the freedom to choose your own doctors and the security of knowing exactly what your healthcare will cost each year, Plan G is the smartest choice for your retirement.
If you have a home in Arizona and would like a quote or have questions on Medicare Plan G we can help!
Ocean McIntyre goes through a file folder of health insurance claims and denial letters at her home in Panorama City on Feb. 10, 2026. (Jules Hotz for KQED)
When Ocean McIntyre started having vision problems at age 34, her health plan took a month to authorize a doctor visit.
When pressure in her brain started crushing her optic nerve, she spent three months tangled in bureaucratic red tape before the insurer finally permitted her to see a specialist, a neuro-ophthalmologist.
“He said if you had been seen earlier, we could have preserved your vision,” McIntyre remembered. “Now we’re just trying to see if we can save any of your vision. That was the first time it really clicked that the life that I had before was over.”
After a wide-ranging career as a tattoo artist, a private pilot, and a research assistant at NASA’s Jet Propulsion Lab near Pasadena, McIntyre is now 51, legally blind and struggling to find work. “I have no peripheral vision at all. It’s like looking through a straw, and what I see is semi-clear in one eye and completely blurry in the other,” she said. “I fall, I trip on things all the time, even in my own house. I’m obviously not flying anymore, not driving a car anymore.”
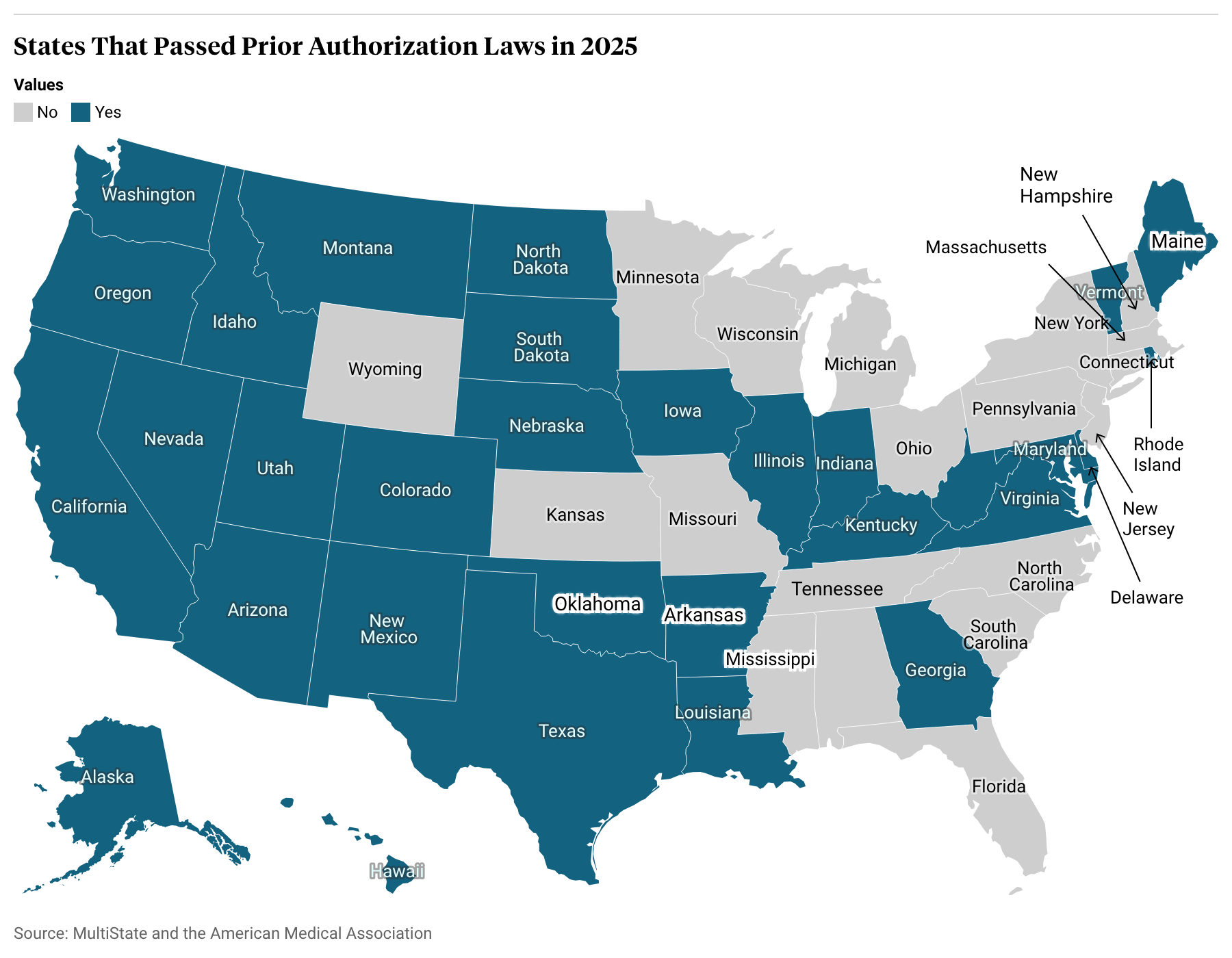
For decades, patients like McIntyre and their doctors have pressed California and other state lawmakers to rein in health insurers’ ability to review or refuse coverage for medical services after a physician has ordered them, a practice known as prior authorization. But the conversation shifted in December 2024 when Luigi Mangione allegedly murdered UnitedHealth CEO Brian Thompson, using bullets etched with the words “delay” and “deny.” The next year, an unprecedented 31 states, at least, passed laws limiting the use of prior authorization, almost all with bipartisan and near-unanimous support.
In 2025, 31 U.S. states passed prior authorization reforms. (Map: Marnette Federis/KQED)
While momentum for legislative change had already been building, several industry insiders and observers said the assassination of an insurance executive, and especially the public outcry that followed, was the catalyst that pushed so many laws over the finish line in 2025. Tens of thousands of people took to social media to both condemn the violence and to air their grievances about insurance tactics and barriers to care.
“It really highlighted for the country this amount of anger,” said Miranda Yaver, health policy professor at the University of Pittsburgh. “And I think that placed pressure on state legislatures.”
Health insurers felt the pressure, too, as lawmakers complained during committee hearings about their own experiences with prior authorization before voting in favor of local bills.
By summer 2025, a coalition of insurance companies issued a pledge to voluntarily streamline, simplify, and reduce the use of prior authorizations. Especially where state legislation aligned with these principles or was narrowly tailored, the insurance industry was more receptive than it had been in the past. Where there was still friction, insurance lobbyists stated their objections, but often struck a conciliatory tone.
Paul Markovich, president and CEO of Ascendiun, the parent company of Blue Shield of California, testifies before the House Committee on Ways and Means with other health insurance CEOs on Capitol Hill, in Washington, on Jan. 22, 2026. (Jose Luis Magana/AP Photo)
“Prior authorization process today sucks. We all take accountability for it,” saidPaul Markovich, CEO of Blue Shield of California, at a congressional committee hearing in January featuring a panel of five health insurance executives. “We are fixing it by reducing the number of services that are covered, offering an online service, and standardizing electronic submission of data.”
Prior authorization started out as a tool insurers used to control costs and tosafeguard patients against unnecessary or harmful treatments. It is typically applied to high-cost items, like experimental treatments, hospitalizations and surgeries, and certain prescription drugs.
For example, back surgeries are often denied because clinical trials show they provide little to no benefit to people who suffer from back pain compared to exercise and physical therapy. Brand-name medications can often be replaced with equally effective, but significantly cheaper, generic alternatives.
Two health insurance denial letters lie on Ocean McIntyre’s table, at her home in Panorama City. Many more are stored in boxes and file folders of communication letters from her health insurance on Feb. 10, 2026. (Jules Hotz for KQED)
“These efforts help keep coverage as affordable as possible,” said Chris Bond, spokesperson for AHIP, a national trade association for the health insurance industry.
But in more recent years, doctors complained that insurers were abusing prior authorization, applying it to more services or using it as a tactic to delay and deter patients away from care. In a 2024 national survey, doctors said they and their staff spent an average of 13 hours a week dealing with prior authorization requests; 23% of doctors said their patients had been hospitalized because of prior authorization delays, 18% said they’d experienced a life-threatening event, and 8% said a patient suffered permanent disability or death.
The mountains of paperwork and constant second-guessing by insurers drive burnout and push doctors into early retirement, said René Bravo, a pediatrician in San Luis Obispo and president of the California Medical Association.
“There is nothing that causes physicians’ blood pressure to elevate like prior authorization,” he said. “You just say the word, and doctors bristle.”
California targets insurance companies
States are taking different approaches to regulating the insurance industry’s use of prior authorization. Some, like Nebraska and North Dakota, focused on expediting the process, mandating timelines for when reviews must be completed, while others restricted the use of artificial intelligence in making determinations.
Many states, including Texas, Arkansas, and West Virginia, have instituted “gold card” programs that exempt doctors from prior authorization if the treatments they order already have a high rate of approval. Others, including Rhode Island and Montana, focused on exempting certain treatments, such as preventive care, insulin, mental health and substance abuse treatment, or some cancer care.
David H. Aizuss, M.D., F.A.C.S., an ophthalmologist and chair of the board of trustees at the American Medical Association, in his office in Encino, California, on Feb. 10, 2026. (Jules Hotz for KQED)
“The California law is different. It puts the onus on the health plans,” said David Aizuss, an ophthalmologist in Los Angeles and chair of the board of trustees at the American Medical Association, which has been tracking state legislation.
SB 306 said that if a health insurer approves a medical service more than 90% of the time in one year, then it can’t require prior authorization for that service the next year.
“This creates a data-driven, common-sense approach,” said state Sen. Josh Becker, D-Menlo Park, who authored the bill. “If you’re approving it anyway, don’t make patients, providers jump through hoops.”
Though attempts to pass a previous version of this bill petered out in 2023, Gov. Gavin Newsom’s office was particularly involved in the passage of SB 306, mediating differences between doctors who supported it and insurers who opposed it, and directing the state Department of Managed Health Care to offer technical assistance.
The regulator is leading the implementation of the law. By July 2026, officials will instruct insurers on how to report the statistics that will be used to list procedures and medications that will be exempted from prior authorization, which regulators expect to publish by July 2027.
Aizuss believes a range of medications for hypertension, diabetes, asthma, and arthritis will make it onto the list, as well as certain outpatient mental health treatments and cancer surgeries.
He’s hopeful that California’s broad approach will lead to more overall transparency and be more effective than other states. Insurers have found loopholes to skirt around the requirements of gold card laws, he said, and the burden is on doctors to prove they should be exempt from prior authorization. For example, in Texas, only 3% of doctors have qualified for gold card status, Yaver said. The California law, by contrast, requires insurers and regulators do the legwork. “This is a positive step toward relieving physician administrative burden,” Yaver said.
Whatever the approach, McIntyre is relieved to see progress in California and across the country. She said no one should suffer a heart attack or a cancer relapse, or lose their vision, because they had to wait for care.